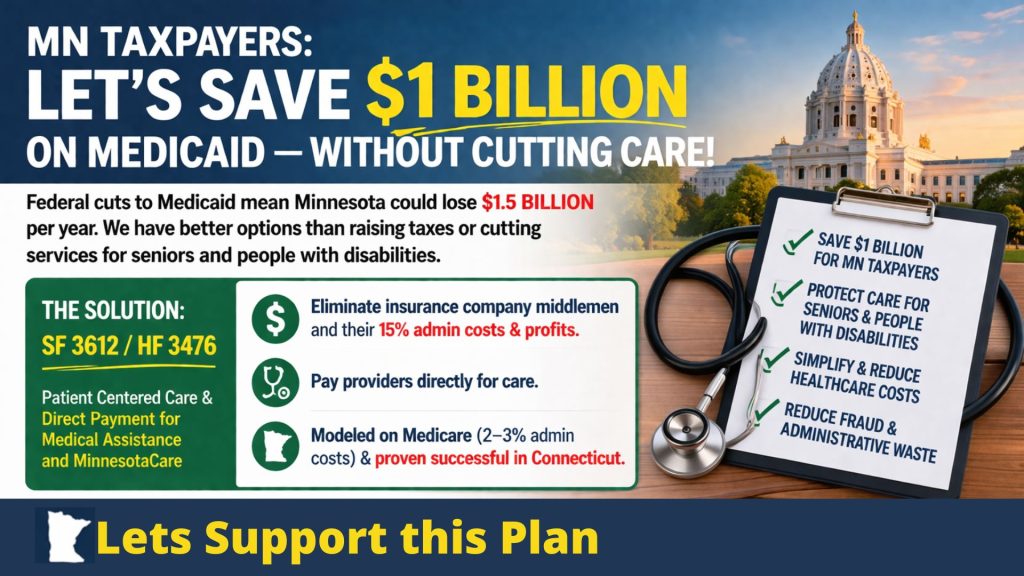

The federal H.R.1 (the One Big Beautiful Bill) that Congress enacted in 2025 cuts $1 Trillion from Medicaid in the next 10 years. That translates to $1.5 Billion less to the State of Minnesota per year. We have three choices:
- Raise taxes by $1.5 billion per year.
- Reduce the services to very low-income seniors and disabled people who are relying on these services to save the $1.5 Billion.
- Find another way to save all or part of that $1.5 Billion.
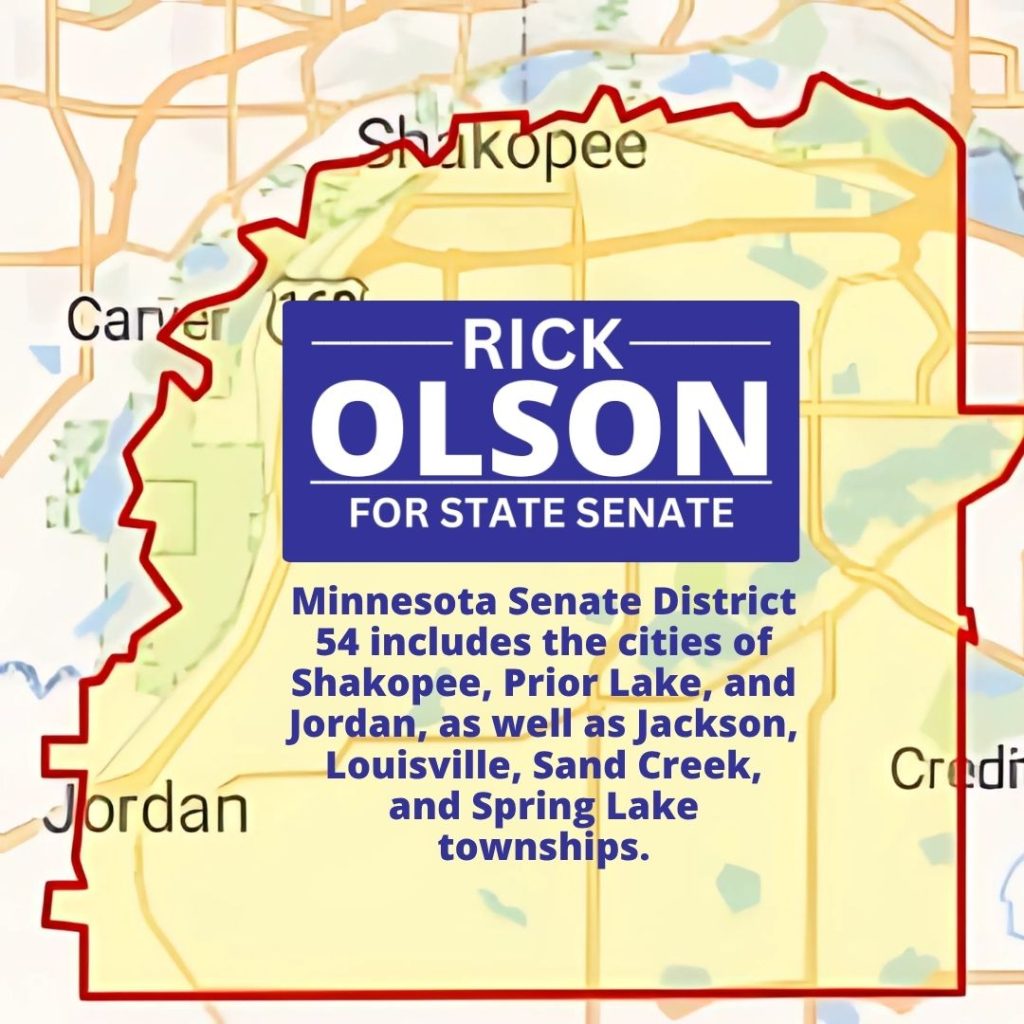
SF 3612 sponsored by Senator John Marty in the Senate and HF 3476 sponsored by Representative Tina Liebling, in the House would save $1 Billion of that $1.5 Billion. With the equally divided House this year, this will likely die in this 2026 legislative session. But, with a strong DFL showing this November, including my winning to retain a DFL majority in the Senate, we can get this done in 2027.

The bills are called “Patient Centered Care and Direct Payment for Medical Assistance and MinnesotaCare”. (Medical Assistance is what we call Medicaid for very low-income seniors and disabled people. MinnesotaCare is a health insurance program for other Minnesotans with low incomes.)
Under these bills, the state would select a private Administrative Service Organization (ASO) which would adjudicate the patients’ claims submitted by the providers. The ASO would pay medical providers (clinics, doctors, hospitals) directly for the care they deliver to patients. This eliminates the use of the current health plans as middlemen and their 15% administrative costs and insurance company profits.
Current estimates are that this would save about 13% of the total cost of the services, netting the $1 Billion. A more detailed report from an exhaustive study of this option requested by the legislature in 2024 is expected early this summer. Obviously, this is a big step and needs to be done carefully.
Q: Can this be done successfully? Connecticut made a similar change. Their successful results are what the13% is based on. This is also similar to how Medicare works with 2-3% administrative costs.
Q: Is this a total solution? No, but saving $1 Billion is nothing to sneeze at and would reduce the extent options 1 and 2 would be needed.
Q: Is this socialized medicine? No, this is simply a single payer system for these covered individuals. The medical providers would not change, but would be unburdened from the enormous complexity and overhead caused by the insurance industry.
Q: Would the coverage provided by this plan be changed from what those covered qualify for now? No, but patients would not have to (1) deal with insurance paperwork, (2) worry whether a provider is in the insurance company’s network, (3) need to reenroll when there are changes in the plans offered from year to year, or (4) suffer from unfair rejected authorizations that their doctors say they need.
Q: Will this cure the problem of between 25 and 30% of total healthcare costs being the administrative costs caused by the health insurance companies? This problem would continue with private insurance purchased directly by taxpayers (or their employers) or through Minnesota’s health insurance marketplace MNsure. So, no, but it is a great step in the right direction.
Q: Will this help reduce fraud? Probably, as the greater the complexity of a system or the number of entities involved, the greater the opportunities for fraud. This is simpler, more transparent and more accessible for AI fraud prevention programs to sniff out potential problems.
By supporting me, you will help provide not only one vote in the Senate but also help retain the DFL majority in the MN State Senate, which is necessary to make this a reality.